Introduction:
At Physio Needs Academy, our commitment to compassionate care extends to families dealing with developmental dysplasia of the hip (DDH). DDH, formerly known as congenital dislocation of the hip, is a condition affecting the hip joint’s congenital or developmental alignment. We aim to provide valuable insights into DDH and offer guidance on its management, ensuring the best possible outcome for your child.
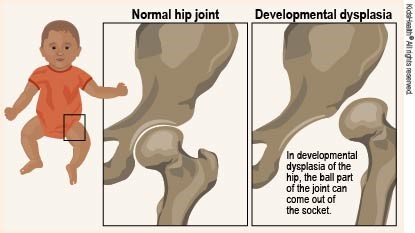
Understanding Developmental Dysplasia of the Hip:
DDH can manifest in various forms, from subtle misalignments to severe deformities or dislocations of the hip joint. It may affect one or both hips, and early detection and intervention are crucial.
Causes of DDH:
DDH is often present at birth, but it can also develop during a child’s first year of life. Recent research has shown that swaddling infants too tightly with straightened hips and knees may increase the risk of DDH. Proper swaddling techniques are essential to prevent this condition.
Signs and Symptoms:
Detecting DDH in infants and children requires vigilance. Signs and symptoms may include:
- Popping or clicking sounds from the baby’s hips.
- Uneven leg lengths.
- Limited hip mobility.
- Misaligned skin folds under the buttocks or on the thighs.
- A noticeable limp when the child begins to walk.
Risk Factors:
Certain factors may increase the likelihood of DDH, including being a first-born girl, breech birth during the third trimester, or a family history of the condition.
Diagnosis:
Diagnosing DDH involves imaging tests such as ultrasound for infants under six months and X-rays for older babies. Early diagnosis is crucial to initiate treatment promptly.
Treatment Options:
Treatment methods for DDH depend on the child’s age and the severity of the condition.
Nonsurgical Treatment:
- Newborns: Infants may wear a Pavlik harness for 1 to 2 months, promoting proper hip alignment and socket development.
- 1 month to 6 months: Similar to newborns, babies can benefit from harnesses or abduction braces, often worn full-time for at least 6 weeks and part-time thereafter.
- 6 months to 2 years: Older babies may undergo closed reduction procedures and spica casting. Skin traction may be used before repositioning.
Surgical Treatment:
- 6 months to 2 years: If closed reduction fails, open surgery is required. Surgeons make an incision at the hip to address the issue. A spica cast is often used post-surgery.
- Older than 2 years: For older children with worsening hip instability, open surgery may be necessary, followed by spica casting.
Recovery and Physiotherapy:
Physiotherapy plays a crucial role in recovery. It can involve gentle traction to facilitate hip bone movement, low-impact exercises like swimming and cycling to enhance strength and flexibility, and physical therapy to improve joint alignment.
Complications and Outcomes:
Complications may arise during treatment, including skin irritation from harnesses and minor growth disturbances. However, with timely and appropriate care, children with DDH can develop normal hip joints and function, avoiding long-term complications like pain and osteoarthritis.
Conclusion:
At Physio Needs Academy, we prioritize compassionate care for children and families navigating the challenges of DDH. Early detection, appropriate treatment, and supportive physiotherapy can pave the way for a brighter, pain-free future for your child. We are committed to providing guidance and resources to help families manage DDH effectively and ensure their child’s well-being.